العربية
Search
Search
About Autism
What is autism spectrum disorder
What is autism
Autism symptoms
Service Centers
Diagnosis
Causes of autism
Service centers
About us
About us
Autism Center of Excellence by Numbers
Board of Directors
Accreditations
Tour
Our services
Rehabilitation services
Evaluation sessions
Therapy sessions
Consulting programs
I train my child
Vocational qualification program
Home care services program
Shadow Teacher Program
Consulting service for establishments
Awareness and education programmes
Subscribe in Padel classes
Consultation session with a consultant doctor
Diagnostic Service
IQ Test Service
Training
Training course for parents
Families Together to Support My Child training program
Parents’ workshops
Workshop for Mothers of Children with Autism Spectrum Disorder
Training course for specialists
ABAT Course
Virtual courses ( online )
Workshop How to Use the Sensory Processing Measure and the Sensory Processing Measure – Preschool
PIVOTAL RESPONSE TRAINING (PRT)
Resources center
Articles
Video
Audio
Books
Researches
Autism podcast
All resources
Partners
Founding donors
Sponsers
Media center
Latest news
Social media posts
Periodicals
Store
Career & Training
Contact us
Menu
العربية
Contact us
The bathroom and its importance as part of daily life skills
Home
The bathroom and its importance as part of daily life skills
The registration in this course is closed
خصم التميز
خصم 20 % لعملاء بنك الرياض
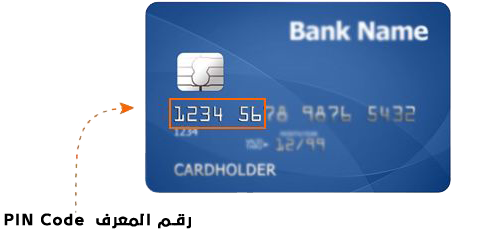
استخدم كود معرف العميل
Search
About Autism
What is autism spectrum disorder
What is autism
Autism symptoms
Service Centers
Diagnosis
Causes of autism
Service centers
About us
About us
Autism Center of Excellence by Numbers
Board of Directors
Accreditations
Tour
Our services
Rehabilitation services
Evaluation sessions
Therapy sessions
Consulting programs
I train my child
Vocational qualification program
Home care services program
Shadow Teacher Program
Consulting service for establishments
Awareness and education programmes
Subscribe in Padel classes
Consultation session with a consultant doctor
Diagnostic Service
IQ Test Service
Training
Training course for parents
Families Together to Support My Child training program
Parents’ workshops
Workshop for Mothers of Children with Autism Spectrum Disorder
Training course for specialists
ABAT Course
Virtual courses ( online )
Workshop How to Use the Sensory Processing Measure and the Sensory Processing Measure – Preschool
PIVOTAL RESPONSE TRAINING (PRT)
Resources center
Partners
Founding donors
Sponsers
Media center
Latest news
Social media posts
Periodicals
Store
Career & Training
Contact us