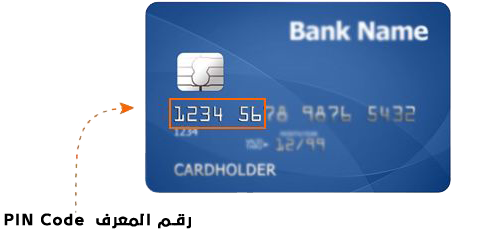
لايوجد لديك صلاحيات للوصول لهذا النموذج Full Arabic Name * ID Number * First English Name * Last English Name * Age * From 5 Years to 12 yearsFrom 12 Years to 18 yearsOver 18 Years Full name of Parents * Email * Mobile 9665XXXXXXXX * Chose the programm that you want * Program for developing communication and social interactionProgram for use the WC Has the beneficiary been registered at the Autism Center of Excellence before? * Yes No Have you been diagnosed with autism spectrum disorder or developmental disorders? * Yes No ماهو نمط التدريب المفضل لديك ؟ * حضوريعن بعد How did you learn about the Center of Excellence for Autism and its services? * Scioal MediaBy a friendThrough a previous beneficiary of the center's servicesThrough one of the center's employeesBy Google Search Other Please enter the ID officer Please agree to the terms and conditions. To view the terms and conditions, please click * Yes I Agree View Terms and Conditions Pay If you are human, leave this field blank.